Laparoscopy: Origins and Applications
Laparoscopic examination of the human abdominal cavity represents a dramatic advance of modern medicine. It is a routine diagnostic procedure used by physicians around the world. How did laparoscopy develop and why is it so valuable? This article will explore both the advancement and practical applications of this remarkable surgical tool.
Image
Laparoscopy is the viewing of intra-abdominal organs via a small abdominal incision utilizing a special viewing scope. This is typically done under an anesthetic. The use of small cameras provides extensive visualization of the abdominal organs, which can also be observed by the assistant staff on television screens. Additional instruments can be placed using similar small incisions to allow various surgical procedures to be accomplished. Surgical procedures that once required a major abdominal incision in the past can now be done laparoscopically via tiny incisions. Laparoscopy has also allowed us to peer into the amazingly coordinated, interconnected, and interdependent anatomy of the abdominal organs. This highly complicated but well-organized and well-functioning system reflects the mind of its creator.
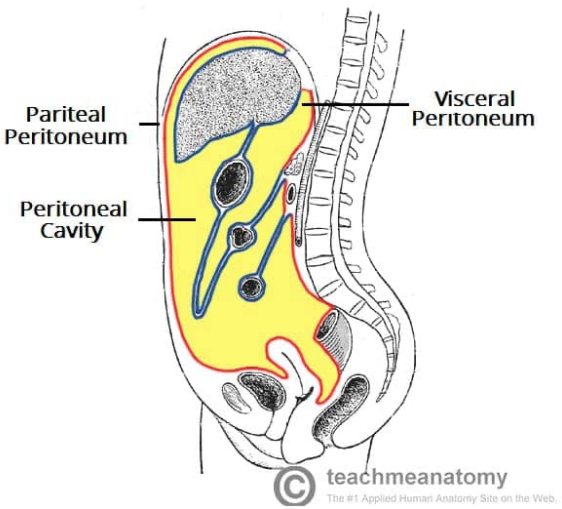
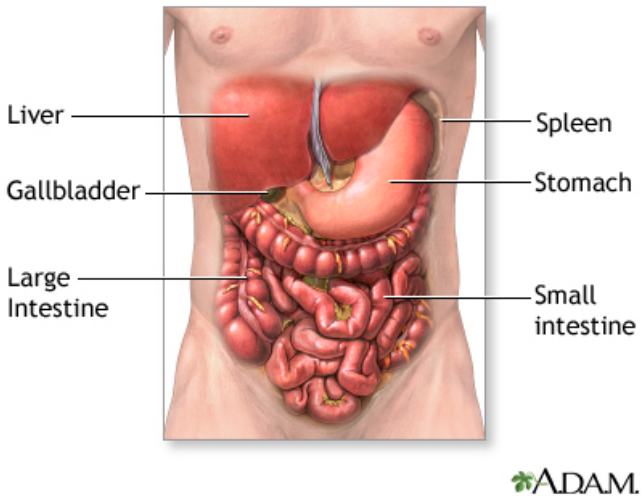
A brief study of human anatomy will allow the understanding of how laparoscopy is possible and how the surgeon can proceed with the examination. The abdominal viscera (liver, spleen, stomach, intestines, etc.) are attached to the body cavity via blood vessels, ligaments, and other thin tissues along the posterior aspect of the abdomen. The attachments to the back wall anchor the viscera in position. (The liver is anchored in the right upper abdomen, the spleen in the left upper abdomen, and so forth.) The anterior aspects of the abdominal organs have no attachments to the abdominal wall. The anterior aspect, being clear of anatomic connections, allows safe placement of instruments and scopes without disruption of the viscera itself. See figure 1. 1 2
Image
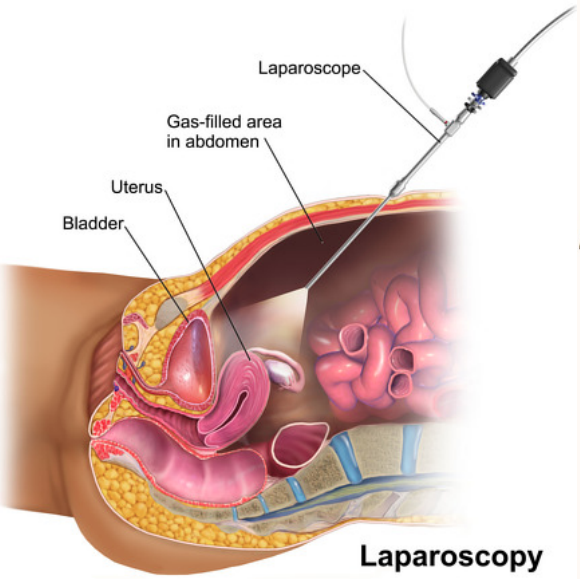
Laparoscopic examination is accomplished by inflating the abdominal cavity with carbon dioxide and placement of cameras or scopes through the abdominal wall musculature. (Inflating the abdomen with carbon dioxide is analogous to opening the hood of a car to check the engine, that is, viewing space is created.) Instruments can be used to view, biopsy, surgically clip, cut, and even suture the abdominal organs. See figure 2 on placement of instruments. 3 4
Image
Image
The first human laparoscopy was done in Sweden by Hans Christian Jacobaeus and was published in 1910. Jacobaeus used a metal trocar (long tube-like instrument) inserted into the abdominal cavity under local anesthesia. He was able to directly visualize the liver in patients with advanced liver disease. His “laparoscopic” approach avoided the need for open abdominal surgery to visualize the liver, an important advantage which persists to this day.
Much of the laparoscopic surgery done during the mid-twentieth century was done by gynecologists. Operations including tubal ligations, excisions of pelvic cysts and ovaries, and management of tubal pregnancies were included in the repertoire of practicing gynecologists. 5 A major change developed in the late 1980s and early 1990s with the introduction of laparoscopic resection of the gallbladder (cholecystectomy). Professor Muhe of Boblingen, Germany and Philippe Mouret of Lyon, France performed the first laparoscopic cholecystectomies in 1985 and 1987, respectively. 6 Cholecystectomy is a very common surgical procedure (more than one million per year in the United States), 7 and the laparoscopic approach expanded quickly through the rest of the world. Laparoscopic resection of the gallbladder rapidly developed as the standard of care for hospitals throughout the nation.
Over the following years (1985-present), laparoscopic surgical instrumentation and surgical expertise have advanced steadily. Surgical courses that taught new laparoscopic procedures and surgical postgraduate programs that specialized in laparoscopy appeared in many academic centers. Emergency appendectomies are now approached laparoscopically on a routine basis. Hernia repairs, small bowel resections, splenectomy, nephrectomy, adrenalectomy, and colon resections have been introduced as common laparoscopic procedures. Even procedures including liver resection and pancreatic resection (initially thought to be prohibitive for a laparoscopic approach) are done in many hospitals.
Laparoscopic surgery has allowed faster recoveries from surgery. Operations that required in-hospital care and long recoveries in the past can now be accomplished with short hospitalizations and faster return to health. For example, colon resections done in the open surgical era often required seven-to-ten-day hospitalizations for recovery. Nowadays, patients with colon resections often leave the hospital in three to five days with considerably less pain. 8 Table 1 is a compilation of common abdominal laparoscopic procedures done in hospitals across the United States.
| Appendectomy | Cholecystectomy |
| Hernia repairs | Small bowel resection |
| Colon resections | Gastric bypass for obesity (bariatric) |
| Placement of dialysis catheters | Correction of gastric reflux disease |
| Liver biopsy | Small bowel obstruction |
| Splenectomy | Nephrectomy |
| Adrenalectomy |
It would be cumbersome to examine each of the above-named laparoscopic procedures in a review article such as this. However, because laparoscopic cholecystectomy is the most frequently performed laparoscopic procedure, this will be briefly reviewed.
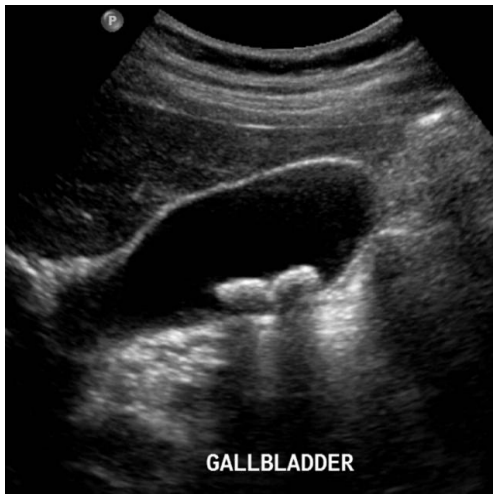
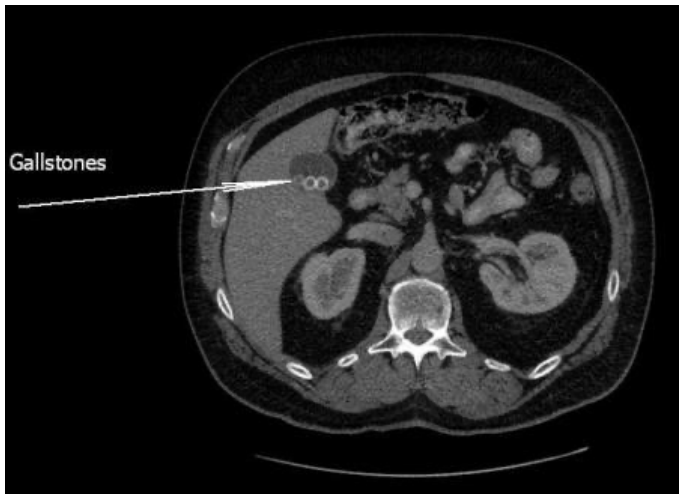
The gallbladder is a common source of abdominal pain, nausea, bloating, and fatty food intolerance. The offending cause is typically gallstones that have formed inside the gallbladder itself. The diagnosis is made when symptoms lead to diagnostic studies such as ultrasound or CT scans which demonstrate gallstones. The management of the disease is removal of the gallbladder (along with the indwelling gallstones) which is done laparoscopically. See diagnostic ultrasound and CT scan studies in figure 3. 9 10
Image
Image
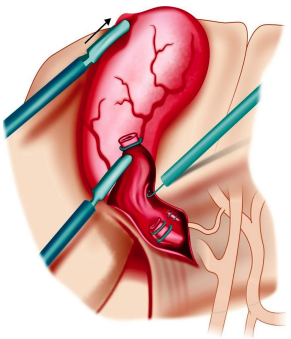
Anatomically the gallbladder is attached to the inferior aspect of the liver. The laparoscopic procedure includes careful division of tissue attachments between the gallbladder and liver. Surgical clips are used to control both the main artery going to the gallbladder and the gallbladder connection to the main bile duct (cystic duct). All this must be accomplished without injuring the liver or other organs and without bleeding. Once the gallbladder is completely free of attachments, it is removed through one of the small incisions. The abdomen is allowed to deflate, and the incisions are all closed. Patients are sent to a recovery area and can go home on the same day as their surgery. The risk of complications is low but can increase if gallbladder inflammation is severe and the surgery is done as an emergency.
Laparoscopic cholecystectomy replaced the traditional open surgical incisional cholecystectomy in the early 1990s. Gradually many other surgical procedures followed suit and became approached laparoscopically as well. The laparoscopic revolution improved the way surgery was practiced. The small incisions allowed shorter hospitalizations, less postoperative pain, faster recovery, and less expense for the medical system.
The laparoscopic revolution has also allowed an unprecedented opportunity to visualize the anatomy and function of the abdominal organs. The laparoscopist can directly see the numerous connections and interactions between each structure. Each organ has its own function which supports and interacts with the others. The complexity and the efficiency of the system is awe-inspiring. The abdominal organs process food intake: saving what is needed and eliminating what is not. Food is chemically altered into useful components which are subsequently distributed to the rest of the body. Each organ is supported by its own arterial blood supply and venous drainage. Each organ communicates with other organs via nerve connections and hormones. Can such complexity develop randomly without an intelligent source? The answer is no.
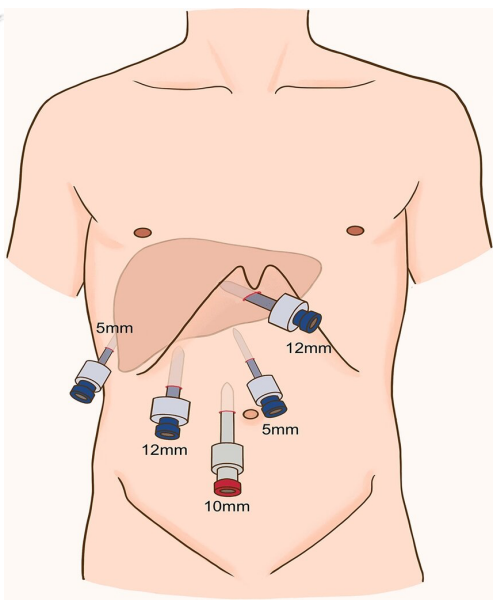
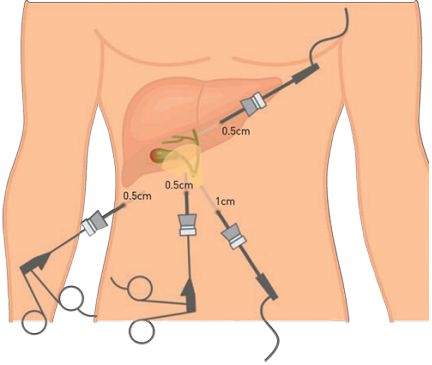
Cholecystectomy begins like all laparoscopic procedures, with inflation of the abdomen and insertion of surgical instruments. The abdomen is inflated with carbon dioxide. (Carbon dioxide is quickly absorbed by the body when the procedure is completed.) The surgical instrumentation includes a scope with a television camera, grasping devices, cutting instruments, instruments that coagulate small blood vessels, and clipping devices to control larger vessels. Each instrument is inserted via a small incision. See figure 4. 11 12
Image
Image
God has allowed man to develop devices that reveal the magnificence of His creation. The Hubble Space Telescope and the James Webb Space Telescope have produced beautiful photos of the most distant stars and galaxies. The Large Hadron Collider in Switzerland has peered into the building blocks of matter: subatomic particles of matter being revealed. Voyager 1 and 2 space probes have examined our own solar system, exploring and photographing the most distant planets. The Laser Interferometer Gravitational-Wave Observatory has been able to sense gravity waves of the universe for the first time. God has given us ample opportunity to ponder and admire His creation.
King David lived approximately 1000 years BC, but he had a keen understanding and appreciation of God’s creation. In the Psalms, David states:
Psalm 8:1 You have set your glory in the heavens. 13
Psalm 146:6 He (God) is the maker of heaven and earth, the sea, and everything in them.
Psalm 139:13 You knit me together in my mother’s womb.
Paul expresses very well the lesson of God’s creation in Romans: 1:20, “For since the creation of the world God’s invisible qualities—his eternal power and divine nature— have been clearly seen, being understood from what has been made.” The laparoscope is another device through which we can admire God’s handiwork. d
- 1 a b O’Neill K (2024 Apr 16) The peritoneum. In Teach Me Anatomy [Internet] https://teachmeanatomy.info/abdomen/areas/peritoneum/ Accessed 2024 Dec 13
- 2 a b MedlinePlus [Internet]. Bethesda (MD): National Library of Medicine (US); [updated 2020 Jun 24]. Abdominal exploration — series — Normal anatomy [updated 2024 Mar 31] https://medlineplus.gov/ency/presentations/100049_1.htm Accessed 202 Dec 13
- 3 a b Smith H, Knipe H, Bell D, et al. (2021 Nov 17) Postoperative free intraperitoneal gas. Reference article, Radiopaedia.org (https://doi.org/10.53347/rID-59318) https://radiopaedia.org/articles/postoperative-free-intraperitoneal-gas Accessed 2024 Dec 12
- 4 a b Zhengm Z, Xie H, Liu Z, Wu X (2022) Laparoscopic central hepatectomy using a parenchymal-first approach: how we do it. Surg. Endo. 36(11):1-9, https://www.researchgate.net/figure/Trocar-placement-A-trocar-for-scope-is-placed-on-the-right-of-umbilicus-a-5mm-trocar-is_fig1_363583681 Accessed 2024 Dec 13
- 5Nakayama DK (2017) The minimally invasive operations that transformed surgery. Bulletin of the Surgical History Group Papers from the 2017 Poster Competition, 64–71. https://www.facs.org/media/xuqgdukk/2017_shg_posterpapers_fullinteractive.pdf Accessed 2024 Dec 13
- 6McClusky D Laparoscopic cholecystectomy. In: SAGES [Internet] https://www.sages.org/wiki/laparoscopiccholecystectomy Accessed 2024 Dec 13
- 7Jones MW, Guay E, Deppen JG (2023 Apr 24) Open cholecystectomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan. https://www.ncbi.nlm.nih.gov/books/NBK448176 Accessed 2024 Dec 13
- 8WakeMed [Internet] What to expect. https://www.wakemed.org/care-and-services/gastroenterology/treatmentsand-procedures/colorectal-surgery/what-to-expect Accessed 2024 Dec 13
- 9 a b Dixon A, Gallstones. Case study, Radiopaedia.org https://doi.org/10.53347/rID-9558 , https://radiopaedia.org/cases/gallstones-1 Accessed on 2024 Dec 13
- 10 a b CT scanning. In: ImageCare [Internet], Medical Imaging, https://imagecaremedicalimaging.communitycare.com/services/ct-scanning/ Accessed 2024 Dec 13
- 11 a b Laparoscopic cholescystectomy. In: SingHealth. https://www.singhealth.com.sg/patient-care/conditions-treatments/Laparoscopic-Cholecystectomy-HPB Accessed 2024 Dec 13
- 12 a b Mishra RK Laparoscopic cholecystectomy operative technique. In: World Laparoscopy Hospital. https://www.laparoscopyhospital.com/iranianmedicaluniversity.htm Accessed 2024 Dec 13
- 13Holy Bible, New International Version®, NIV® Copyright ©1973, 1978, 1984, 2011 by Biblica, Inc.®